

The Medical Humanities Society at Des Moines University presents its first annual online arts gallery, “Another Season Comes and Goes.” The gallery features art works and the written word by DMU students depicting seasons of human life and of the earth.
Gallery curators are Megan Kavanaugh, a second-year osteopathic medical student, and Megha Pokhriyal, a first-year osteopathic medical student. They are executive officers of the Medical Humanities Society.
| Part 1 | View the full series | Part 3 |
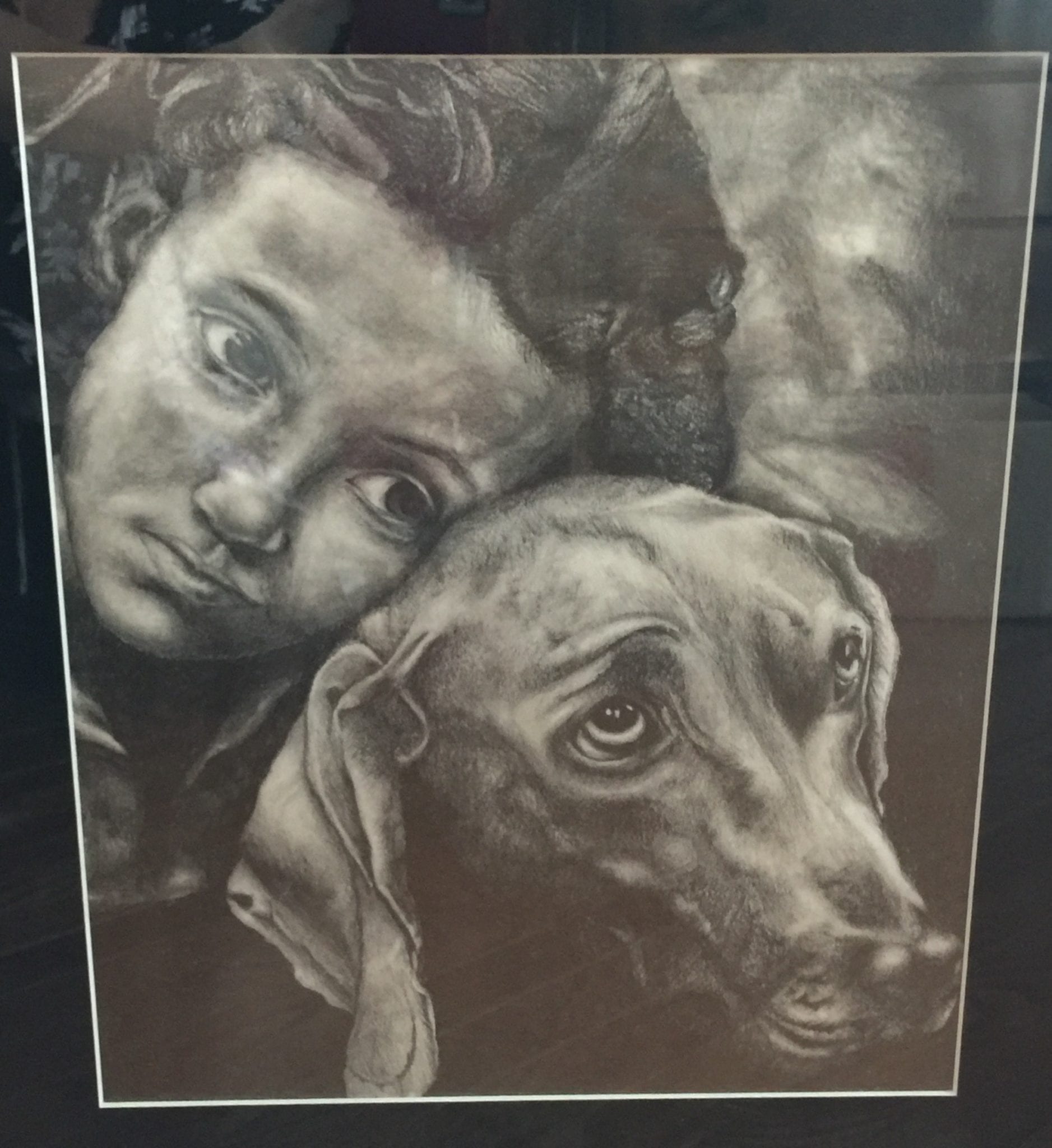
Today we feature works by two students. The drawing below is by Amanda Buck, a second-year osteopathic medical student from Chicago. “This is a pencil drawing of a picture I came across,” she says. “When I saw the picture, I was most impressed with the love I saw for a little girl and her dog. Growing up with a dog, I understood this love, which for me was unconditional and constant. It’s one of the most beautiful relationships I feel blessed to have experienced.”
Featured below is a short story by Andrew C. Schroeder, a third-year osteopathic medical student from St. Louis, MO. He describes the inspiration for his story as follows: “I was surprised by the range of emotions I felt during my first real code situation as a medical student. I sensed the same thing from many of the people in the room. It is such a unique and live experience, obviously not common to a normal 9-5 job. I wanted to describe what I saw and felt, and hopefully process some of the emotions. In the end, as I think the story shows, our goals are the same as the patient’s goals, and whatever route our emotions take us to get there is just fine.”
Night Shift
My first overnight shift during my first clinical rotation as a third-year medical student in the Emergency Department: the nervous anticipation had been building all afternoon. Of course, nothing really tangible separates a day shift from a night shift, except perhaps a feeling of well-restedness on the first of a long series of night-shifts. The anticipation, however, like something big is going to happen, is near tangible. I suppose things are always more dramatic at nighttime.
The call came around 11 p.m. A man was found down. EMS was transporting, resuscitating and calling to announce their imminent arrival. The Emergency Department, at a baseline din of background activity, lurched into action. A nurse opened the trauma-bay doors. Another guided the name-brand, multi-million-dollar medical boom along its slick-gliding track out of the way to facilitate entry of a stretcher into the room. Dr. K took note of the call while moving to inform a patient of a just-received test result. He absorbed the information over his shoulder as he moved away, returning just moments later with a quick inhalation and a glance my way.
We moved toward the trauma bay, and a nurse asked me if I had ever done chest compressions before. This was it. The night-shift experience I had been anticipating. The nervous anticipation turned to nervous excitement. Did I sense the same from Dr. K? Was that a tiny mischievous smile? This was definitely the reason he chose Emergency Medicine.
Wait a second. What – is that guilt? Yes, I definitely felt a twinge of shame and guilt for rooting for an exciting case and an active role. I tried to hide my smile as the room filled with people in preparation of EMS’s arrival. But then I sensed the same thing in the room, the same muted excitement I felt. A bunch of adrenaline junkies waiting, somewhat respectfully, for the main event. Across the room, Dr. K cracked a quiet joke as he donned his gloves, releasing some of the pressure from the room. He caught my eye and moved closer to impart some wisdom on his student.
“Make sure you have all of your equipment ready,” he said. He wheeled the laryngoscope cart closer. “They probably have secured an airway, but we can’t be sure.”
Nurses who had tucked their patients in for the next few minutes showed up in the doorway, anticipating the start of the chaos. I felt my pulse quicken beneath my gloves and sheer, multi-ply gown. I counted a few breaths as the room, now with 10 or 12 people in it, shifted its weight nervously. Dr. K stood a little taller than I had seen him in the first 5 hours of the shift. EMS arrived.
The wheels of the stretcher squeaked and strained as they rolled through the sliding doors and into the trauma bay. The automatic chest compression device pumped noisily and quickly like a runaway train rhythmically clacking down the tracks. EMS personnel hurried around the stretcher, blurting out the pertinent facts of this man’s story as they transferred him from the stretcher to the Emergency Room bed. He was found down. They do not know for how long. He has had no pulse or respirations since they found him.
The commotion continued for five or six minutes. The man’s skin was mottled and gray. Sadly, although appropriately, nurses and staff began exiting the room as they learned their assistance would not be needed. The nurses in the doorway realized we would not resuscitate this man and made their staggered exits as well.
Dr. K called it, patient pronounced deceased at 11:29, and there were three people left in the room. A purposeful grief replaced the nervous excitement as we removed the medical equipment from the man’s lifeless body. I was unsure how long to stay in the room, and a bit depressed at the anti-climactic end. No chest compressions. No intubation. The guilt returned immediately, for even beginning to feel sorry for myself. But then again, I think, he probably wishes we all could have done more as well.
| Part 1 | View the full series | Part 3 |
